What are “Critical Mad Perspectives’ & Why Do They Matter?
During my graduate studies in social work at Ryerson last year, I did a research project called Centering Sanism – Stories & Visions for Mad Positive Mental Health. Essentially, this was an academic representation of my real-life process of decolonizing* the way I think about, and practice, my community mental health work.
I have worked as a ‘case manager’ with people diagnosed with ‘serious mental illnesses’ for over 25 years. I am also a family member of loved ones diagnosed with mental illnesses. And I have also struggled with some mental health issues of my own – I have come to endearingly refer to them as my ‘moments of madness’. I could do that, because I am protected from psychiatrization by my various privileges – whiteness, long-term employment, middle-class status, mainstream lifestyle, university education, etc … Over the years, I squirmed my way through the question: What is the difference, really, between myself and the ‘clients’ that I work with? And more importantly, why does this matter?
Going back to university as a mature student let me explore these questions further. I started by considering mental health stigma (our negative thoughts), which feeds mental health discrimination (our negative actions), which then causes mental health oppression (our power over others). I landed here, at sanism, and the bigger picture of power inequities embedded in psychiatric ways of knowing. Along the way I learned about Mad Studies, which focuses on the person over psychiatric diagnoses, creating possibilities for redressing oppressions and shifting societal thoughts and practices.
Once you adopt an anti-oppression lens for one issue you start noticing everything from a similar lens, or at least I did. In spite of my newfound enthusiasm about Mad Studies, I soon became aware of its limitations. Specifically, I did not find that Mad Studies adequately incorporated the interwoven oppressions that people with mental health struggles experience, such as those based on race, class, gender, sexuality, and so forth. After all, one’s experiences of struggles and support greatly depend on the body that carries these experiences.
At school, I was fortunate to be surrounded by professors and students who influenced my thoughts around critical race theories, decolonization, queer studies, and anti-black racism. My research project rooted itself in Madness and Mad Studies, but I was uncomfortably aware of who was taking up this discourse – mostly white educated folks like myself. So I added to Mad Studies the lens of intersectionality, along with the lens of critical social work, and the lens of anti-oppression. This is when Critical Mad Perspectives was born for me, and together, these multiple lenses helped me to see things very differently.
Looking at my community mental health work from a Critical Mad Perspective let me uncover the layers of inequities and microaggressions that keep certain bodies marginalized by their mental health experiences, and grant certain bodies the freedom to playfully call their mental health struggles ‘moments of madness’. It opened up possibilities for considering a shift in our community mental health practices that is rooted in ‘Mad-positive’ mental health. This was the basis of the pilot research that I did for my master’s research project.
The participants that I spoke with on this topic were people who identified as ‘peer workers,’ meaning that they held both service provider and service user perspectives. They were eager to share their personal stories and experiences, which informed their own vision for a Mad-positive mental health support system. In a nutshell, research participants saw promise for moving forward in the foundations of community, empathy, and love.
The answer to the question Why Critical Mad Perspectives matter? lies in the overall findings from my research and discussions with participants:
- Intersectionality is overlooked in a pathology approach:
As long as dominant mental health practices rely on a patholigizing approach that labels and treats mental disorders, important social contexts are missed—contexts that relate to what contributes to mental health distress in the first place. Using a lens of intersectionality helps to contextualize someone’s mental health experiences and understand how power, privilege, and oppression operate upon that person.
“Mental health doesn’t just happen to people”
“It’s the isms, the discriminations, the multipleisms.”
“Identity is not a chemical imbalance”
The comments from research participants reinforced the point that mental health issues are not a separate occurrence. Rather, compounding experiences of discrimination are contributors to mental health distress. And intersecting identities make some more vulnerable to pathologization then others.
- Madness is a human rights and social justice issue:
The human rights code is meant to protect everyone with disabilities from discrimination, while social justice seeks fair and equitable treatment of people within society. While these social guideposts shape our lives and are accepted by most people unquestionably, when it comes to mental health disabilities and Madness, there is great resistance to framing these experiences as human rights and social justice issues.
“We are basically the same blood”
“There is this underlying power imbalance”
“Focusing on the brain disease lets everything else off the hook”
Participants are telling us to put humanity front and centre, not diagnosis. Intersecting lived experiences of mental health distress invariably relate to power. Therefore, we need responses that address the whole person and their oppressions.
- Non-clinical mental health practices matter too:
Our current clinical mental health practices stem from psychiatry, which is rooted in modernist constructions of ‘mental illness’ as binary opposite to mental health. When we view mental health experiences exclusively from this clinical, positivist lens, responses are necessarily void of consideration for the complexities of human distress beyond pathology. In other words, there is little space for other ways of knowing in a system that dominates through solutions rooted in diagnosis and medication. Alternatives that do not feed the business of psychiatry will hardly be welcome. Yet research participants were unanimous in naming non-clinical practices as the key to widening our mental health practices and moving forward in ways that have the capacity to make a difference to people marginalized by their mental health experiences.
“There’s lots of different ways that emotional pain, can transpire”
“That is their answer—let’s sedate people”
“It’s not in their interest to divert to non-clinical practices”
De-centering clinical practices means looking beyond one narrow dominant approach that relies predominantly on medicating emotional distress. Participants’ comments raised the question – Where is the space for other methods? By challenging the business of psychiatry, we are making space for non-clinical practices and Madness, in all its critical forms.
This research continues to be front-of-mind for me, even now that I am finished my studies and back to work as a community mental health worker. I am looking for ways that the theory of Critical Mad Perspectives can influence my practice as a social worker, and beyond.
While Critical Mad Perspectives is helping me to dig deeper for the whole person buried beneath confining psychiatric labels, this theory opens up many possibilities for thinking differently about mental health issues and the people affected by them.
In practice, this means moving towards a Mad-positive support system that recognizes oppression in all its forms as a contributor to mental health distress, and that is directed by people’s lived and contextual experiences.
In education, this means ensuring critical mental health discourse at all school levels to challenge the dominant biomedical teachings around mental health, and to foster complex, creative responses for making our society more genuinely inclusive and just.
In research, this means pushing the boundaries of acceptable knowledge to overcome historically imbedded power and rights issues, and influence policy and systemic-level change.
All of this speaks to the possibilities for Critical Mad Perspectives to shift the conversation about Madness and its interlocking layers of oppression. This theoretical framework provides us with a multi-layered lens to examine social issues of all sorts, and to use this as a tool for community building and solidarity in fighting injustices on many levels. Mostly, it is about hope – that by widening our understandings in critically important ways, we will soon target the real sources of mental health stigma, discrimination, and oppression.
Written by Lois Didyk
* decolonizing refers to the process of undoing colonialism, thereby challenging the establishment and maintenance of dominant ways
Lois Didyk is a recent graduate from the Master of Social Work program at Ryerson, and can be reached at ldidyk@ryerson.ca.
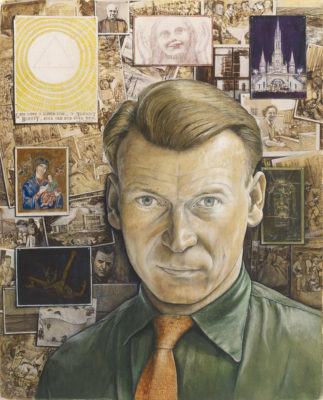 I remember studying a large tableau of Kurelek’s entitled “Don Valley on a Grey Day” (1972) and “Self-Portrait” (1957) which showed a shift from the “portals to his suffering” (4) of his asylum days to his “new post-conversion path” (4). This painting, which glared back at me in AGO’s Thomson Collection (6), shows “a confident and optimistic self” with “narratives [which] are more orderly rather than free-flowing, painted as photographs and postcards neatly stacked to a bulletin board.” (4)
I remember studying a large tableau of Kurelek’s entitled “Don Valley on a Grey Day” (1972) and “Self-Portrait” (1957) which showed a shift from the “portals to his suffering” (4) of his asylum days to his “new post-conversion path” (4). This painting, which glared back at me in AGO’s Thomson Collection (6), shows “a confident and optimistic self” with “narratives [which] are more orderly rather than free-flowing, painted as photographs and postcards neatly stacked to a bulletin board.” (4)